Polycystic Ovarian Syndrome (PCOS)
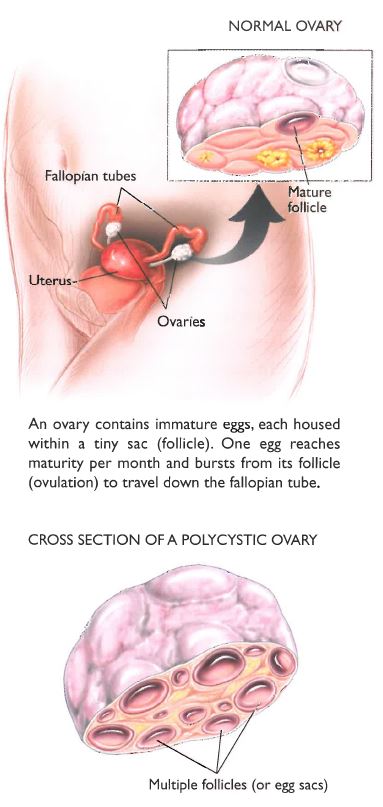
It affects about 10–15% of all women in greatly varying degrees. Many women are totally unaware that they are affected. Normally each month in the ovaries several eggs start to develop for ovulation but only one fully develops and is released.
In women with polycystic ovaries a single egg does not become dominant and lots of eggs, often 15–30 per ovary are growing at once. None of them fully mature for ovulation and instead, they eventually form small cysts (see diagram below).
Thus the normal monthly cycle of egg development, growth, release into the tubes and on into the uterus does not occur. The ovaries continue to produce the hormones oestrogen and testosterone, but the normal burst of progesterone production that follows ovulation does not occur.
Most women with PCOS do not have regular menstrual cycles and do not have regular monthly bleeds. When a bleed does occur it might be due to a burst of normal egg development and a normal cycle, but more commonly it is just an
erratic breakdown of the lining of the uterus after several months of continuous oestrogen production by the ovaries.
Women with PCOS usually describe one or more of the following:
1. Development of infrequent and irregular periods, often during adolescence
2. Sudden weight gain in adolescence or early adulthood
3. Excessive facial and/or body hair (hirsutism)
4. Acne and oily skin
5. Scalp hair loss( androgenic alopecia)
6. Infertility
7. Continuous weight gain or trouble losing weight.
We don’t know what causes PCOS. No single gene abnormality has been found in PCOS but probably several different gene combinations result in this condition.
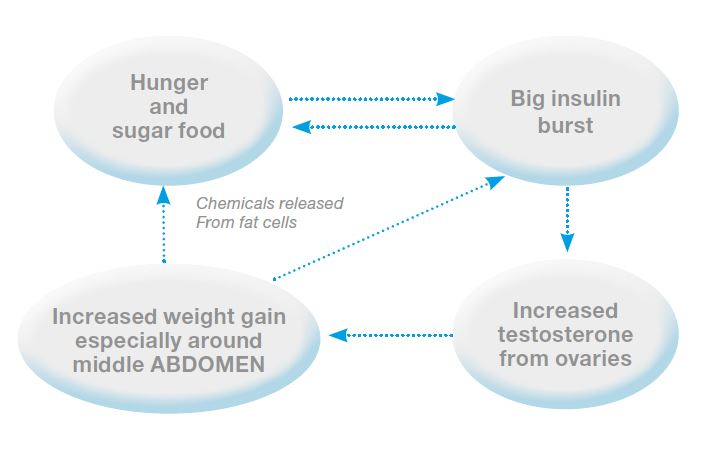
The ovaries of women with PCOS commonly over produce testosterone, resulting in extra hair growth and/or acne. Another common feature of PCOS is a tendency to need to make more insulin than normal to control blood sugar. Therefore after eating sugary food, women with PCOS are likely to have a much greater burst of insulin than women without PCOS.
The high blood insulin also acts on the ovaries to make more testosterone. Thus a cycle of weight gain stimulating increased hormone levels which then further stimulates weight gain occurs.
Tests
Blood tests: these may all be completely normal or a woman with PCOS may be found to have:
1. High blood insulin when fasting or after a sugar challenge (oral glucose tolerance test);
2. High levels of testosterone or DHEAS (a hormone made by
the adrenal glands, that can be converted to testosterone); and
3. A low level of the protein that binds to the sex hormones called sex hormone binding globulin (SHBG).
Ultrasound
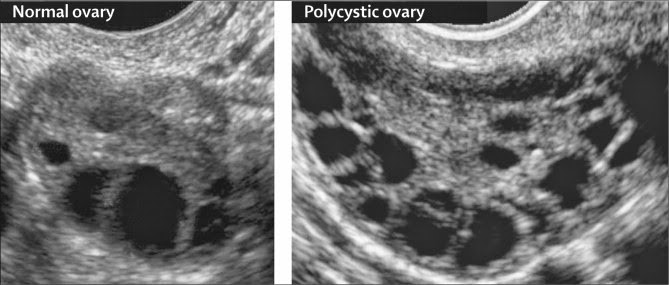
An ultrasound study can be performed to see the size and appearance of your ovaries. The typical appearance of an ovary affected by PCOS is lots of small cysts mostly towards the outside of the ovaries. More than 15 cysts (follicles) per ovary is considered typical of PCOS.
Treatment of PCOS
Weight management is a common problem and this needs to be primarily addressed by diet and exercise, although medication may sometimes help.
Women should avoid sugary foods to reduce stimulating big bursts of insulin release. Women with PCOS who have a high fasting blood insulin, and/or an abnormally high insulin surge after a sugar challenge (oral glucose tolerance test – OGTT) often respond well to treatment with a medication called metformin.
Metformin increases the sensitivity of the body to insulin, so less insulin needs to be made, and the abnormal cycle is interrupted. Treatment with metformin is associated with the return of regular menstrual cycles and regular ovulation, and sometimes weight loss as well. This treatment is often used for women with PCOS trying to get pregnant. Metformin may cause diarrhoea. It is generally started at a low dose, with a gradual increase in dose. Women with PCOS who are troubled by acne and excess hair growth may respond to treatment with a class of drugs called anti-androgens such as cyproterone acetate (Androcur) and spironolactone (Aldactone).
Long term effects
There is no cure for PCOS but for women who are overweight the best care is weight control, and ideally weight loss. Women with PCOS who are overweight have a greatly increased risk of developing diabetes after the age of 40 years. Women who have PCOS and don’t have regular periods over several years are at increased risk of uterine cancer. Therefore we recommend treatment to create a regular bleeding cycle.